
Gastroesophageal Reflux Disease(GERD)
According to Wikipedia,
Gastroesophageal reflux disease (GERD) is a chronic upper gastrointestinal disease in which stomach content persistently and regularly flows up into the esophagus, resulting in symptoms and/or complications. Symptoms include dental corrosion, dysphagia, heartburn, odynophagia, regurgitation, non-cardiac chest pain, extraesophageal symptoms such as chronic cough, hoarseness, reflux-induced laryngitis, or asthma. In the long term, and when not treated, complications such as esophagitis, esophageal stricture, and Barrett’s esophagus may arise.
Overview
What Is GERD?
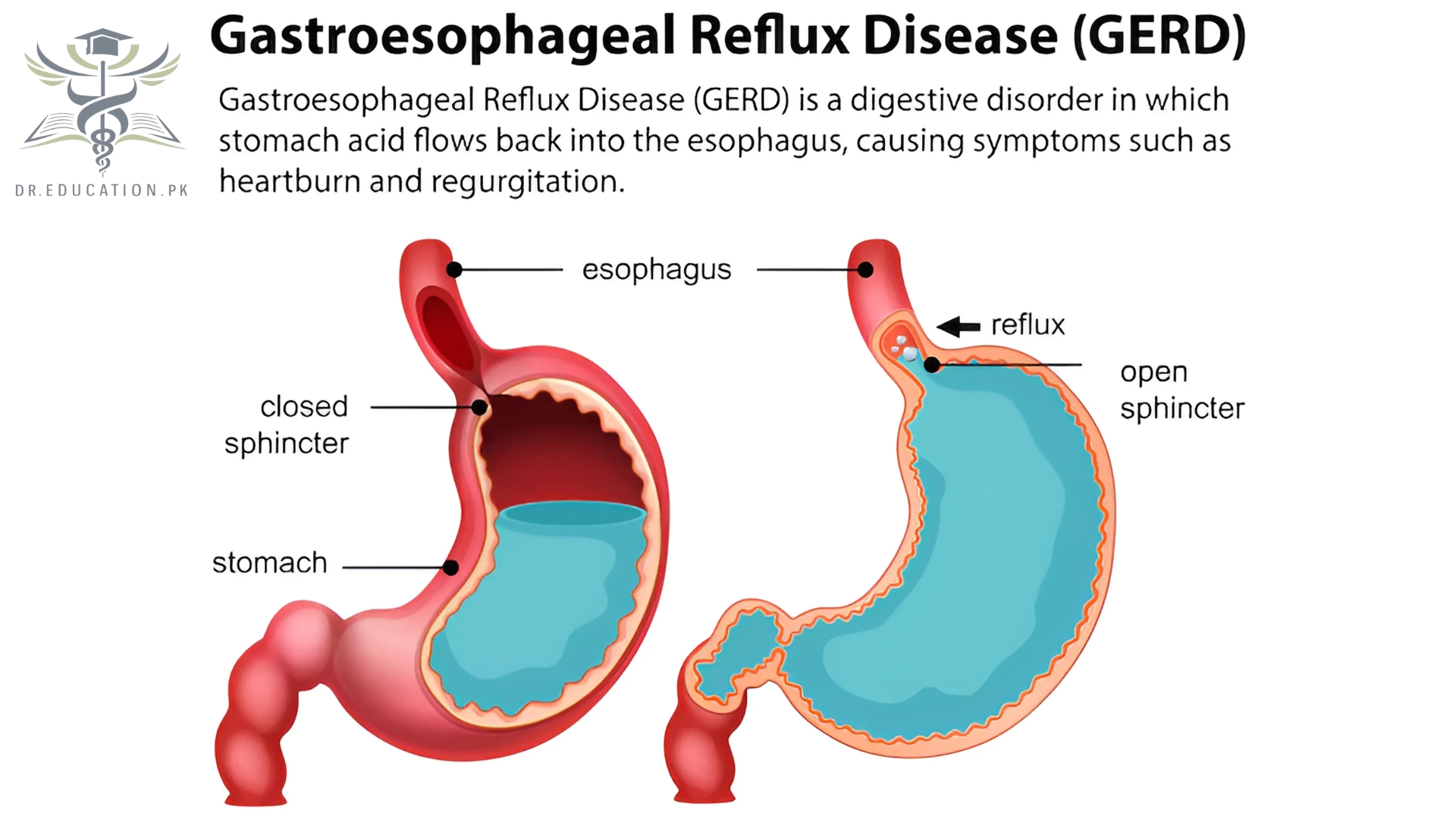
Gastroesophageal reflux disease (GERD) happens when acid from your stomach backs up into your esophagus, the tube connecting your stomach to your mouth.
This digestive disorder affects the ring of muscle between your esophagus and your stomach. This ring is called the lower esophageal sphincter (LES). If you have GERD, you may get heartburn or acid indigestion. Doctors think that some people may have it because of a condition called hiatal hernia. In most cases, you can ease your GERD symptoms through diet and lifestyle changes. But some people may need medication or surgery.
What is acid reflux?
Your stomach contents are supposed to travel only one way: down. When acid from inside your stomach flows backward — meaning, up — into your esophagus and throat, it’s called acid reflux.
When acid creeps into places it doesn’t belong, you’re bound to feel it. Acid irritates and inflames the tissues inside your esophagus, which runs from your stomach up through your chest to your throat.
Almost everyone has experienced an occasional episode of acid reflux. It might feel like indigestion — burning stomach pain after eating — or heartburn — burning chest pain close to your sternum.
Occasional acid reflux is uncomfortable, but it’s not a disease. But some people have reflux all the time. Chronic acid reflux can really affect your quality of life, and it can also do real damage to your tissues.
Symptoms
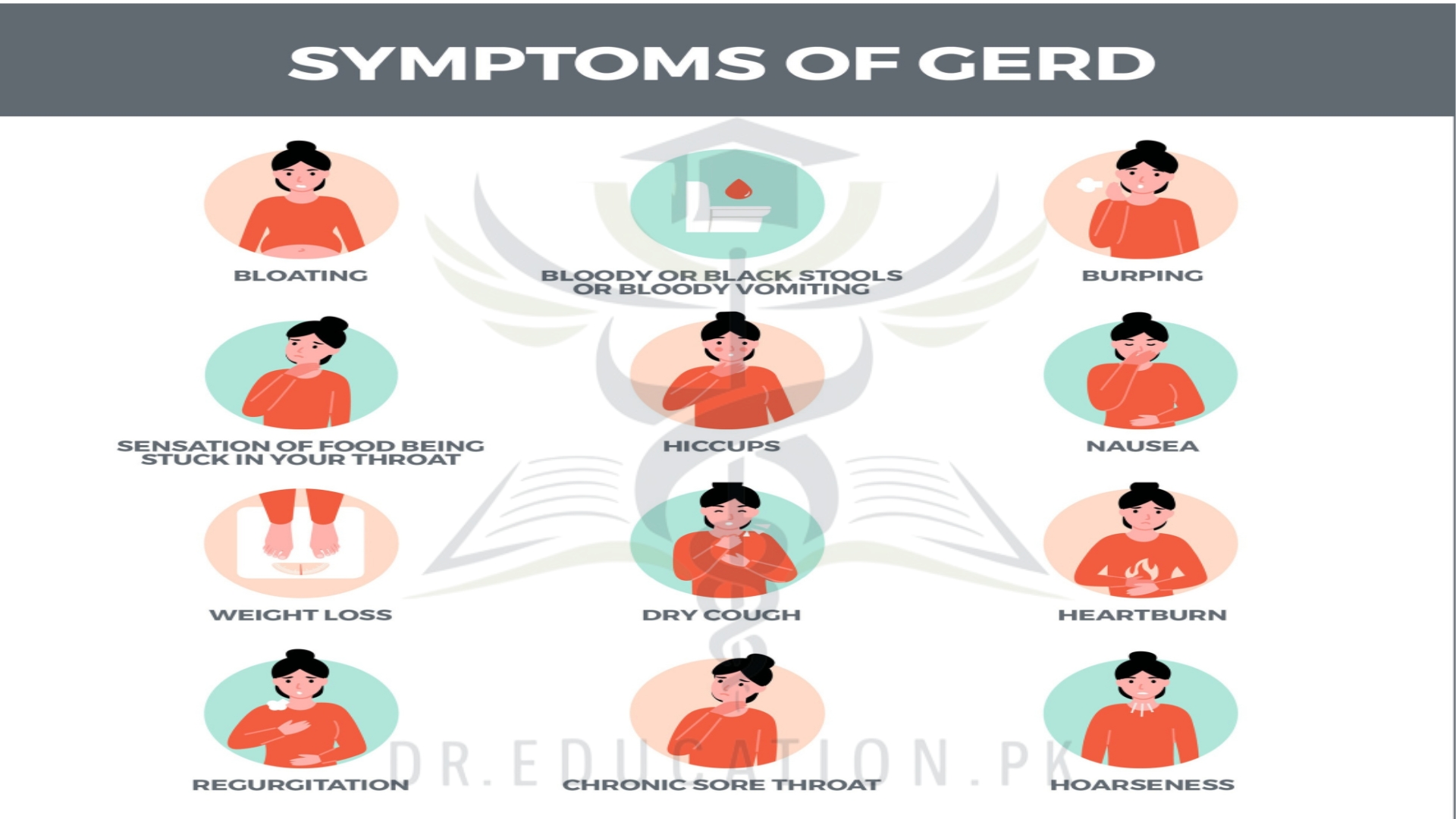
Common symptoms of GERD include:
- A burning sensation in the chest, often called heartburn. Heartburn usually happens after eating and might be worse at night or while lying down.
- Backwash of food or sour liquid in the throat.
- Upper belly or chest pain.
- Trouble swallowing, called dysphagia.
- Sensation of a lump in the throat.
If you have night-time acid reflux, you also might experience:
- An ongoing cough.
- Inflammation of the vocal cords, known as laryngitis.
- New or worsening asthma.
What causes acid reflux?
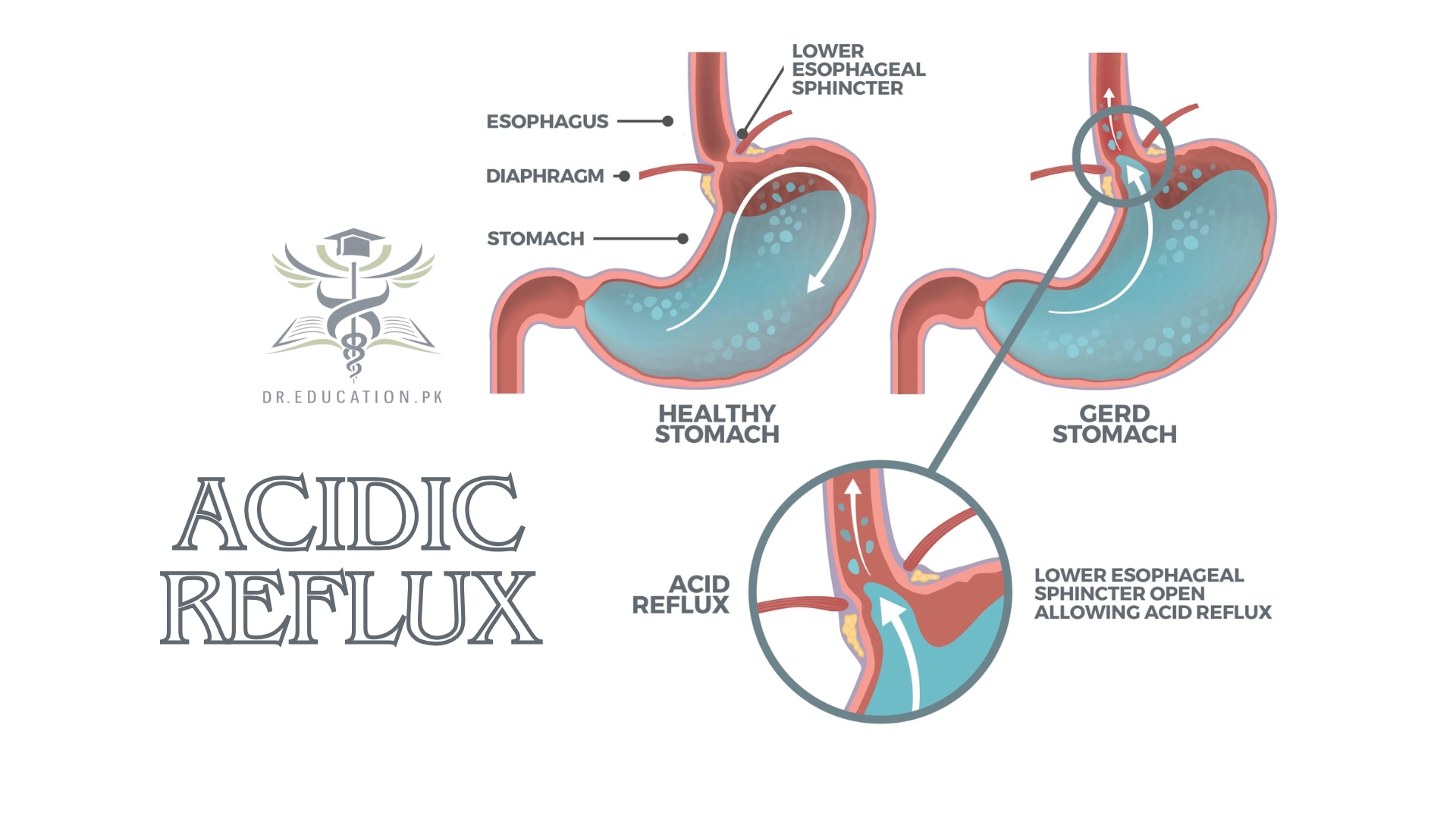
For acid to get into your esophagus, it needs to get past the valve at the bottom of your esophagus that usually keeps things from coming back up. This valve is called your lower esophageal sphincter (LES).
Your LES is a circular muscle that opens when you swallow and then closes again to keep substances in your stomach. It also opens a little to let gas bubbles out when you’re burping or have hiccups.
Acid reflux happens when your LES weakens or relaxes enough to let acid pass. Some temporary things can relax your LES, like lying down after a large meal. But if you have GERD, it means your LES is relaxing often.
Many things can contribute to weakening your LES, either temporarily or permanently. Sometimes occasional acid reflux turns into chronic GERD when these factors overlap or persist for a long time.
Common causes of acid reflux and GERD include:
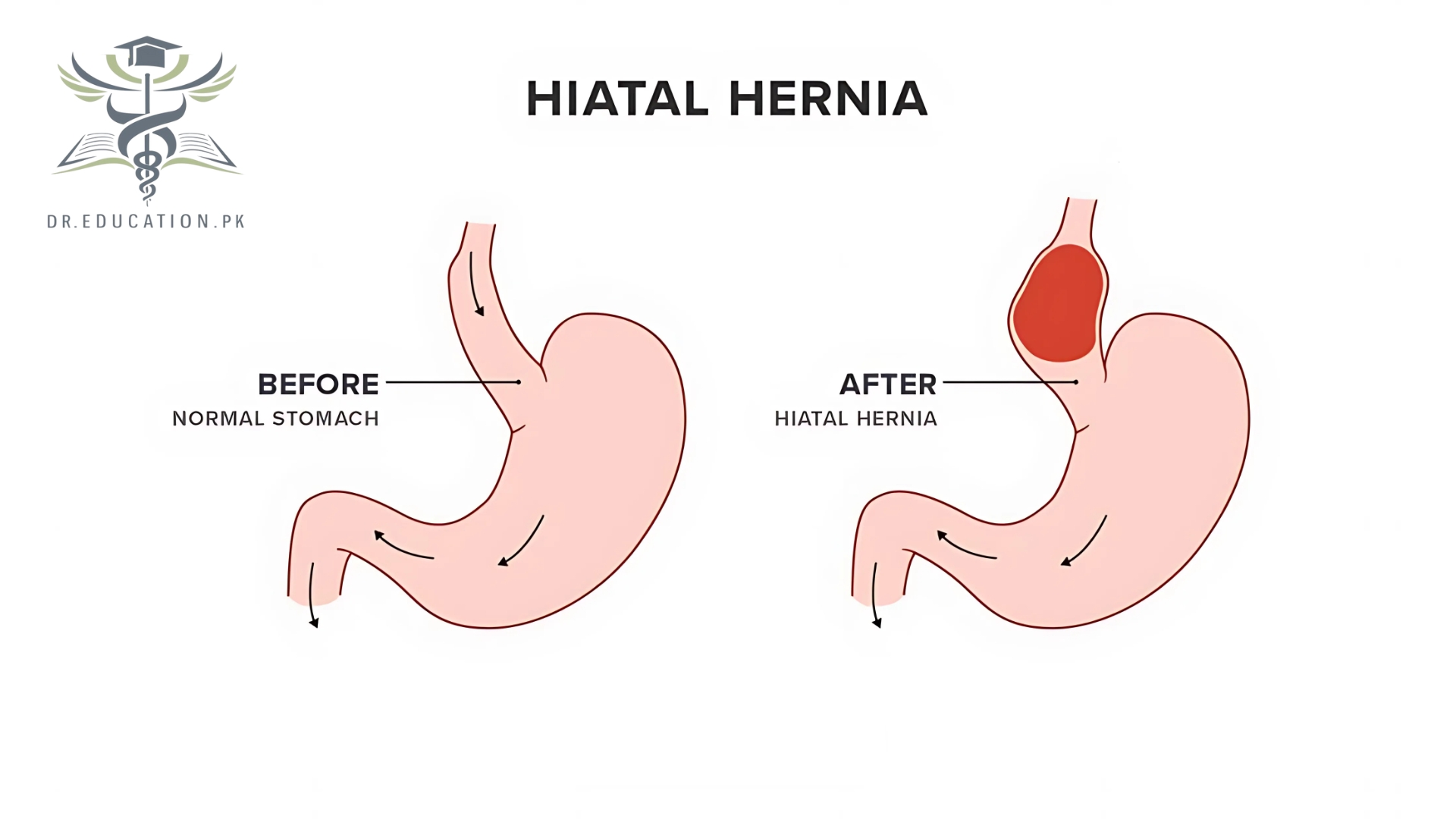
- Hiatal hernia. A hiatal hernia happens when the top of your stomach pushes up through the hole in your diaphragm where your esophagus passes through. It squeezes in next to your esophagus, compressing them both and trapping acid. It also moves your LES above your diaphragm, where it loses some of its muscular support. Hiatal hernias are very common, especially as you get older. They usually occur gradually, and they can gradually worsen.
- Pregnancy. Pregnancy is a common cause of temporary acid reflux. The pressure and volume in your abdomen can push, stretch and weaken the muscles in your diaphragm that support your LES. Pregnancy hormones may also encourage your LES to relax. Pregnancy brings high levels of the hormone relaxin, which relaxes your muscles so they can stretch to make room for the fetus. It also brings high levels of estrogen and progesterone, which may also relax your LES.
- Obesity. Obesity increases the pressure and volume in your abdomen, which affects your LES similarly to how pregnancy does. Obesity also tends to last longer than pregnancy, which can weaken the muscles more permanently. It’s a common contributing factor to developing a hiatal hernia. Since fat tissue secretes estrogen, having more of it also raises your estrogen levels.
- Smoking. Tobacco smoke relaxes your LES, whether you’re the one smoking or you’re exposed to second-hand smoke. Smoking also triggers coughing, which opens your LES. Smoking and chronic coughing can weaken your diaphragm muscles and contribute to developing a hiatal hernia. Smoking also slows down your digestion and causes your stomach to produce more acid.
Other possible causes of GERD include:
Birth defects. Congenital defects like esophageal atresia and hernias can affect your LES.
Connective tissue diseases. Diseases like scleroderma may affect your esophagus muscles.
Prior surgery. Surgery in your chest or upper abdomen may have injured your esophagus.
Medications. Certain medications can have a relaxing effect on your LES, including:
- Benzodiazepines, a type of sedative.
- Calcium channel blockers, which treat high blood pressure.
- Tricyclic antidepressants, which treat depression and pain.
- NSAIDs (nonsteroidal anti-inflammatory drugs) like aspirin and ibuprofen.
- Theophylline, a common asthma medication.
- Hormone therapy (HT) medications for menopause.
GERD in children
Recent studies show that GERD in infants and children is more common than doctors thought. It can cause vomiting that happens over and over again. It can also cause coughing and other breathing problems. Older kids and teens also can have GERD. But it’s more common for young people to have an occasional bout of reflux without it being a more serious or ongoing problem.
Other risk factors for GERD in babies or children include:
- Down syndrome
- Muscular dystrophy
- Cerebral palsy
- Other neuromuscular disorders
GERD Causes
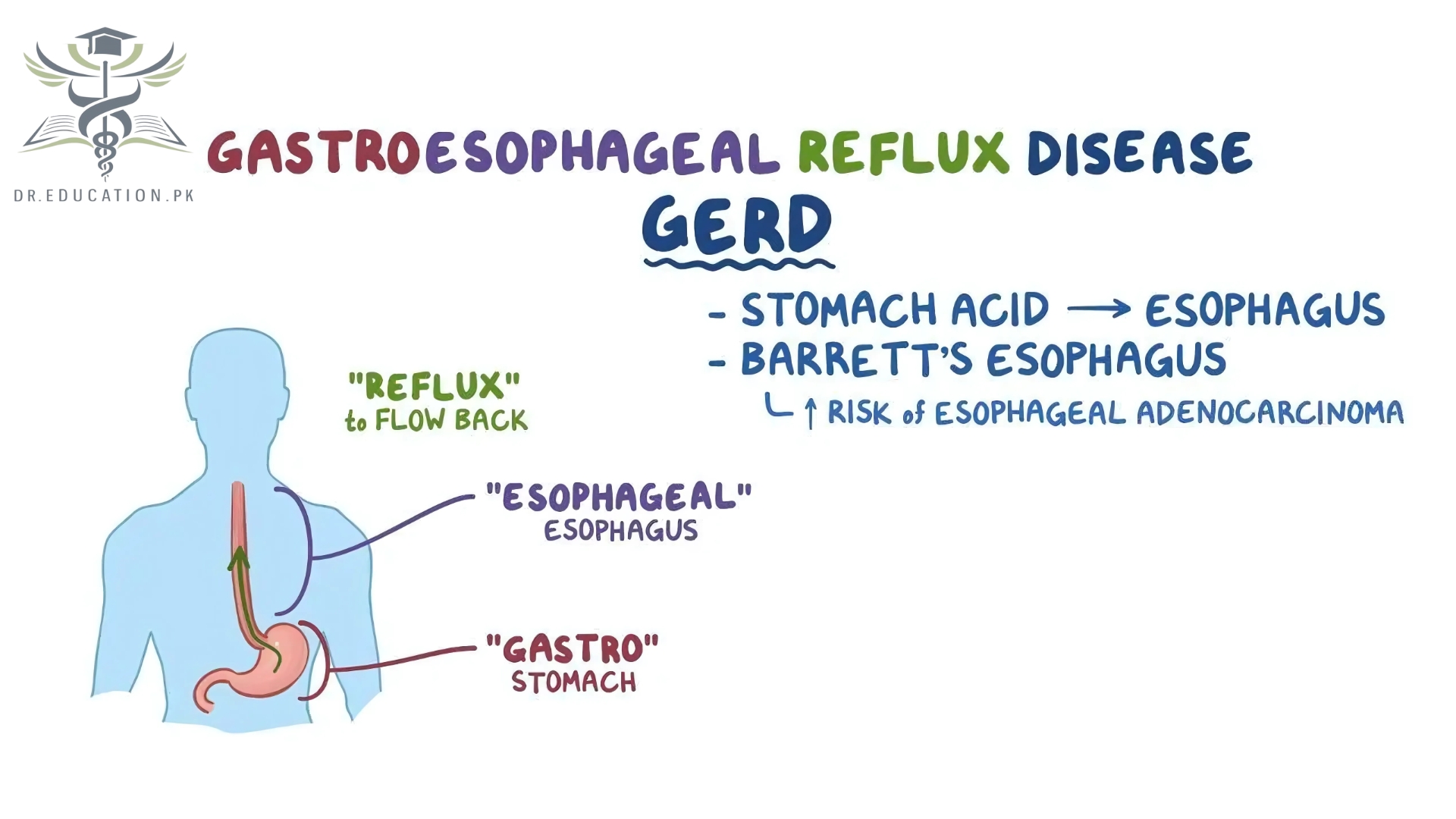
The term “gastroesophageal” refers to the stomach and esophagus. Reflux means to flow back or return. Gastroesophageal reflux is when what’s in your stomach backs up into your esophagus.
In normal digestion, your LES opens to allow food into your stomach. Then, it closes to stop food and acidic stomach juices from flowing back into your esophagus. Gastroesophageal reflux happens when the LES is weak or relaxes when it shouldn’t. This lets the stomach’s contents flow up into the esophagus.
Risk Factors
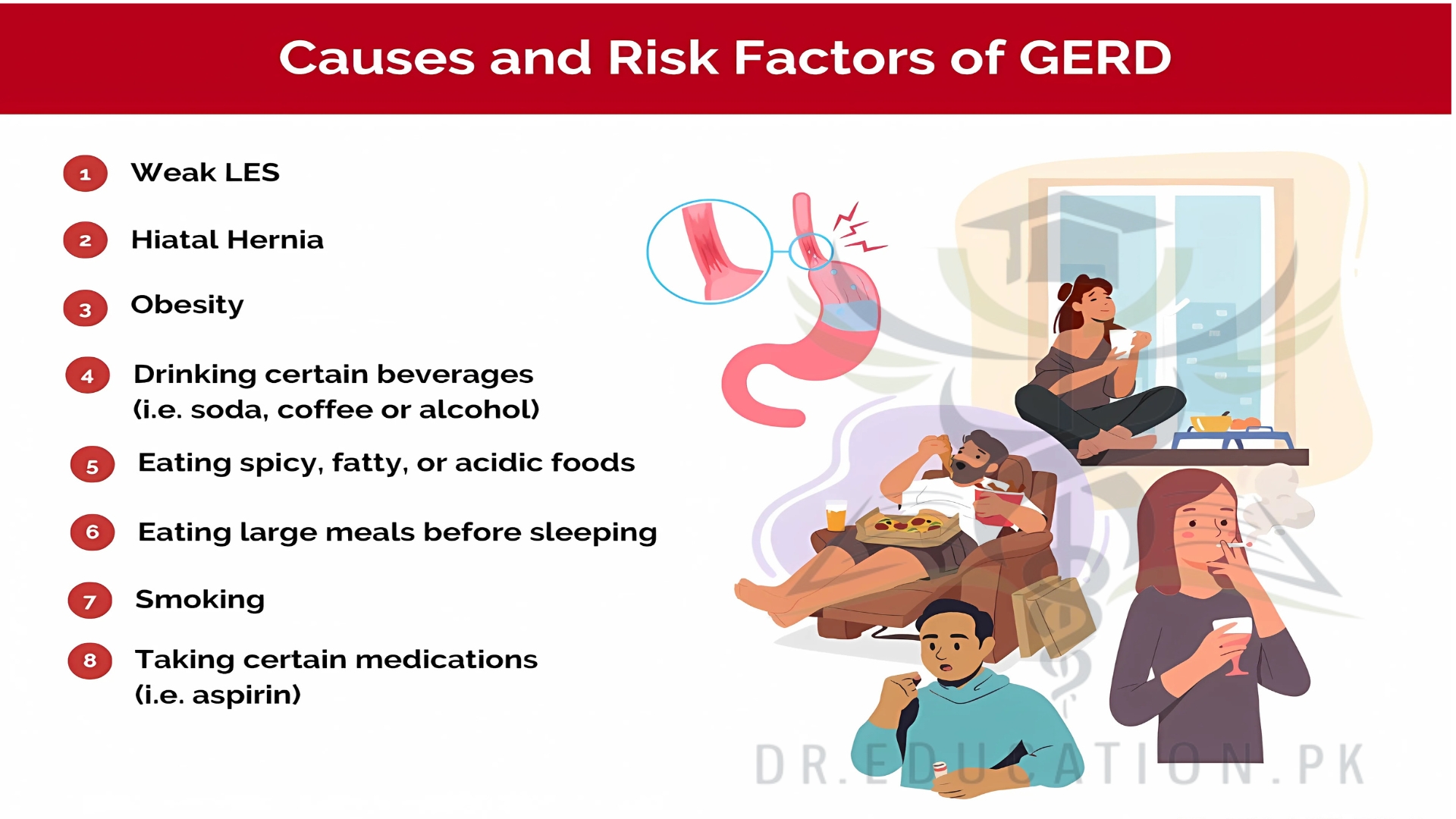
Conditions that can increase the risk of GERD include:
- Obesity.
- Bulging of the top of the stomach up above the diaphragm, known as a hiatal hernia.
- Pregnancy.
- Connective tissue disorders, such as scleroderma.
- Delayed stomach emptying.
Factors that can aggravate acid reflux include:
- Smoking.
- Eating large meals or eating late at night.
- Eating certain foods, such as fatty or fried foods.
- Drinking certain beverages, such as alcohol or coffee.
- Taking certain medicines, such as aspirin.
GERD Complications
Sometimes, GERD can lead to serious complications:
Esophageal ulcer. Stomach acid eats away at your esophagus until an open sore forms. These sores are often painful and may bleed, making it hard for you to swallow food.
Esophageal stricture. Stomach acid damages the lower part of your esophagus and causes scar tissue to form. This scar tissue builds up until it narrows the inside of the esophagus, making it hard to swallow food.
Barrett’s esophagus. Acid reflux changes the cells in the tissue that lines your esophagus. The lining gets thicker and turns red. This condition is linked to a higher chance of esophageal cancer.
Lung problems. If reflux reaches the back of your throat, it can cause irritation and pain. From there, it can get into the lungs (aspiration). If this happens, your voice may get hoarse. You could also have chest congestion and a lingering cough. If your lungs get inflamed, you can develop asthma, bronchitis, and even pneumonia.
How is GERD diagnosed?
A gastroenterologist will evaluate your esophagus to diagnose GERD. Tests may include:
- Esophagram. An esophagram is a type of X-ray exam. It takes moving X-rays (fluoroscopy) of your esophagus while you swallow. For the test, you swallow a chalky liquid called barium.
- Upper endoscopy. An upper endoscopy involves looking inside your esophagus with a camera. The camera is on the end of a thin tube that passes through your mouth while you’re asleep under light sedation.
- Esophageal pH test. This test measures the acid content inside your esophagus through a small wireless receiver. Your provider places the receiver in your esophagus during an endoscopy.
- Esophageal manometry. This test measures the muscle activity in your esophagus, using pressure sensors embedded in a nasogastric tube. It can confirm if your LES or other muscles aren’t working right.
Management and Treatment
What is the medical treatment for GERD?
Some people find they can reduce acid reflux with lifestyle adjustments, like changing their eating habits, reducing alcohol and tobacco and losing weight. Healthcare providers encourage this approach.
But if you have chronic acid reflux or GERD, they also recommend medicines to reduce your stomach acid, so reflux is less damaging. These medicines are easily available and highly effective for GERD.
Medicine
Over-the-counter (OTC) medicines for acid reflux include:
- Antacids. Antacids neutralize your stomach acid so that when reflux happens, it isn’t as corrosive to your esophagus. They work well for occasional acid reflux, but they can have side effects if you take them too often, so they aren’t a good long-term solution.
- Alginates. Alginates are naturally occurring sugars derived from seaweed. They help block acid reflux by floating on top of the acid, creating a physical barrier between the acid and your esophagus. You can get alginates by themselves, and you can also get antacids with alginates.
Prescription medications for GERD include:
- Histamine receptor antagonists (H2 blockers). H2 blockers reduce stomach acid by blocking the chemical that tells your body to produce it (histamine). You can take them more frequently than antacids, but they don’t always work long-term. Your body can adapt to their effects.
- Proton pump inhibitors (PPIs). PPIs are stronger acid blockers that also promote healing. Your provider may prescribe them as a first-line treatment if your GERD is relatively severe or you have signs of tissue damage in your esophagus. They’re 90% effective in reducing acid reflux.
- Baclofen. Baclofen is a muscle relaxant, often prescribed to reduce muscle spasms. It can also help reduce the frequency of LES relaxation events, which reduces the frequency of acid reflux. Baclofen isn’t a first-line treatment for acid reflux, but it may be a part of your treatment plan.
Surgery and other procedures
GERD can usually be controlled with medicine. But if medicines don’t help or you wish to avoid long-term medicine use, a healthcare professional might recommend:
- Fundoplication. The surgeon wraps the top of the stomach around the lower esophageal sphincter, to tighten the muscle and prevent reflux. Fundoplication is usually done with a minimally invasive, called laparoscopic, procedure. The wrapping of the top part of the stomach can be partial or complete, known as Nissen fundoplication. The most common partial procedure is the Toupet fundoplication. Your surgeon typically recommends the type that is best for you.
- LINX device. A ring of tiny magnetic beads is wrapped around the junction of the stomach and esophagus. The magnetic attraction between the beads is strong enough to keep the junction closed to refluxing acid, but weak enough to allow food to pass through. The LINX device can be implanted using minimally invasive surgery. The magnetic beads do not affect airport security or magnetic resonance imaging.
- Transoral incisionless fundoplication (TIF). This new procedure involves tightening the lower esophageal sphincter by creating a partial wrap around the lower esophagus using polypropylene fasteners. TIF is performed through the mouth by using an endoscope and requires no surgical incision. Its advantages include quick recovery time and high tolerance.If you have a large hiatal hernia, TIF alone is not an option. However, TIF may be possible if it is combined with laparoscopic hiatal hernia repair.
What helps acid reflux at home?
To help manage acid reflux at home, try:
- Eating smaller meals. Larger meals expand your stomach and put pressure on your LES. Smaller meals digest faster and don’t stimulate your stomach to produce so much acid.
- Eating dinner earlier. Gravity plays a role in keeping acid down, so it’s a good idea to eat several hours before reclining in the living room or going to bed.
- Sleeping on your left side. This positions your lower esophageal sphincter in an air pocket above your stomach contents. Lying on your back or your right side submerges the valve.
- Reducing abdominal pressure. Wear loose-fitting clothes or consider losing weight if you have overweight/obesity. This can help in the short term and the long term.
- Quitting smoking and drinking. Both tobacco and alcohol weaken your LES. They also affect your stomach, making it more acidic and slowing your digestion time.
- Over-the-counter medications. Antacids and alginates are good to have on hand, especially if you know you’re eating a rich or acidic meal that might trigger more stomach acid.
Conclusion from Dreducation.pk
In conclusion, gastroesophageal reflux disease (GERD) is a complex, chronic condition that significantly impacts quality of life and can lead to serious complications if untreated. GERD symptoms often include heartburn, acid reflux, and discomfort in the chest and throat, which can progressively worsen over time.
Effective management of GERD involves a combination of lifestyle changes, dietary modifications, and in some cases, medication or surgical intervention. By understanding the underlying causes, including factors such as hiatal hernias, obesity, pregnancy, and lifestyle habits like smoking, individuals can take proactive steps to reduce symptoms. Home remedies, such as eating smaller meals, avoiding trigger foods, and adjusting sleep positions, can also alleviate discomfort.
When lifestyle adjustments are insufficient, medical treatments, including over-the-counter antacids, H2 blockers, or stronger proton pump inhibitors, offer effective symptom relief. For severe or persistent cases, advanced treatments like fundoplication surgery or the LINX device provide lasting solutions.
Ultimately, by recognizing the symptoms early and seeking appropriate care, individuals with GERD can manage their condition and reduce the risk of complications, including esophageal damage and Barrett’s esophagus.






