TABLE OF CONTENT
How do you pronounce orthopnea?
What is orthopnea?
What is the difference between orthopnea and dyspnea?
What causes orthopnea?
How is orthopnea diagnosed?
How is orthopnea treated?
Overview
How do you pronounce orthopnea?
Orthopnea is pronounced (or-thaap-nee-uh).
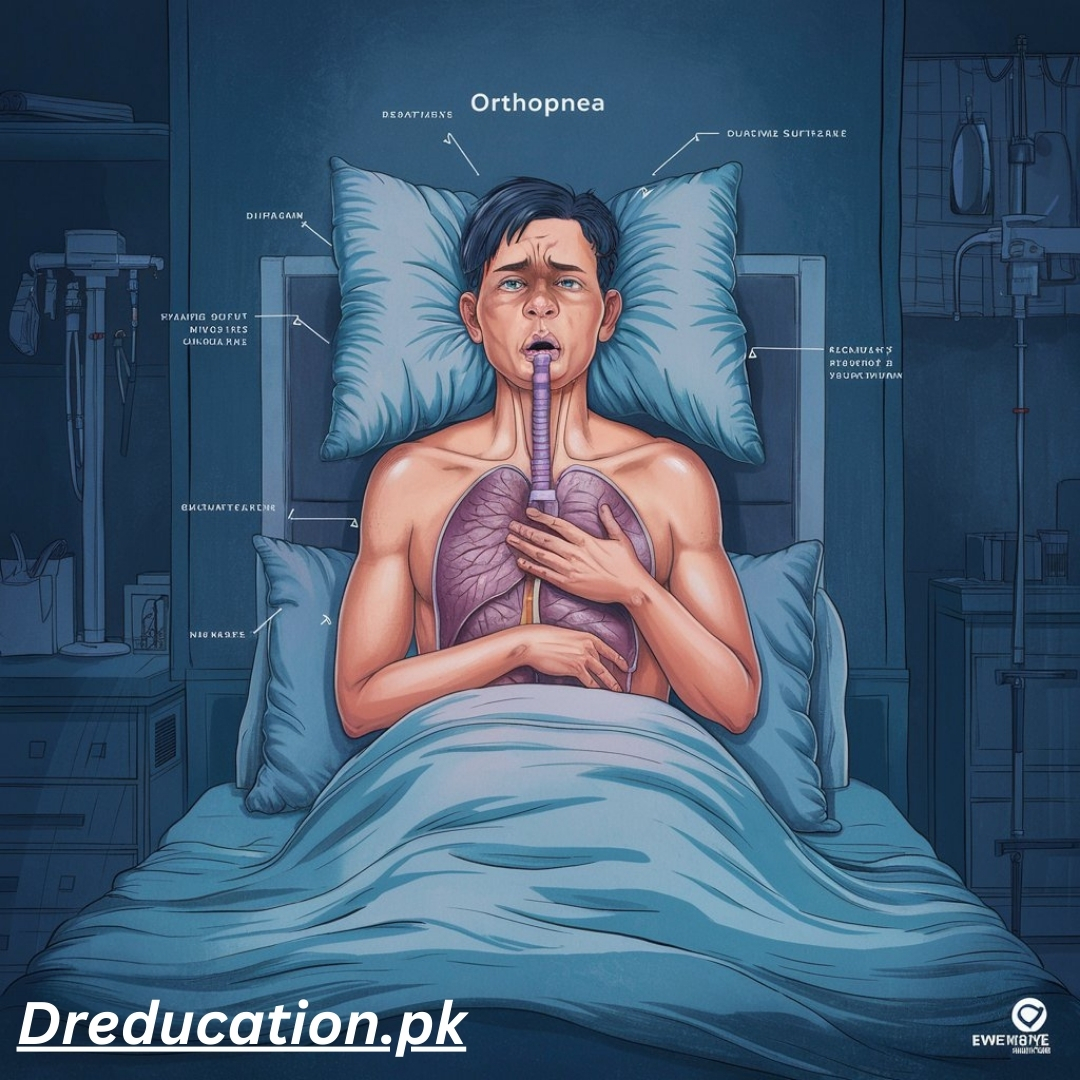
What is orthopnea?
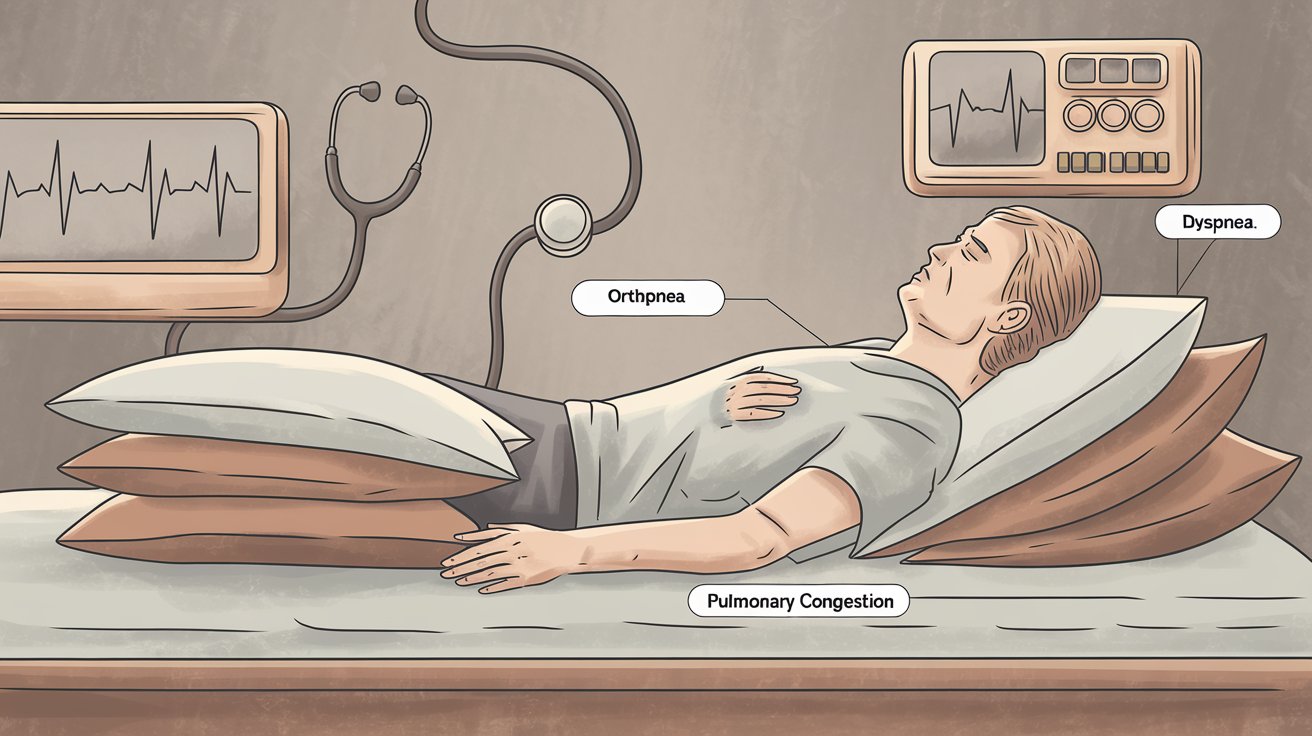
Orthopnea is a medical term to describe shortness of breath that occurs while lying flat and is relieved by sitting or standing. Orthopnea can occur progressively over time or spontaneously, depending on the underlying cause.
Individuals may describe needing to use multiple pillows to sleep due to breathlessness. An increased number of pillows required to sleep may signify a more severe form of orthopnea. For example, three-pillow orthopnea may be more severe than two-pillow orthopnea.
Orthopnea occurs when pulmonary congestion causes the lungs to become stiff and non-compliant, which is when the lungs are unable to stretch and expand to effectively bring in air. When recumbent (i.e., lying flat), pulmonary compliance decreases due to the lungs assuming a more posterior position.
The work of breathing increases as a result of the changes in compliance, which causes a subsequent increase in respiratory rate in order to properly ventilate the lungs. Concurrently, lying down increases the redistribution of blood from the lower extremity and splanchnic blood vessels (i.e., blood flow from abdominal gastrointestinal organs) to the lungs.
The increased blood flow to the heart increases the pressure within the pulmonary blood vessels. In individuals with an underlying disease, the increase in blood volume, increased pressure, and decreased compliance when lying down cannot be overcome, resulting in pulmonary edema and orthopnea.
What is the difference between orthopnea and dyspnea?
Orthopnea and dyspnea both describe when individuals feel short of breath; however, orthopnea specifically refers to shortness of breath while in the supine or recumbent position. On the other hand, dyspnea simply describes shortness of breath.
What causes orthopnea?
Orthopnea may be caused by several underlying conditions. The most common cause of orthopnea is due to heart disease, such as congestive heart failure, coronary artery disease, or valvular dysfunction.
In heart failure or coronary artery disease, the left ventricle may be unable to adequately pump blood into systemic circulation. Blood will then regurgitate into the left atrium and pulmonary circulation, which increases the pressure in the lungs and causes pulmonary edema (i.e., fluid in the lungs).
Additionally, valvular disease, such as mitral stenosis, can also cause fluid to back up into the left atrium and lungs. Those with a history of a myocardial infarction are also at an increased risk of developing orthopnea. Orthopnea is also often caused by chronic obstructive pulmonary disease (COPD), such as emphysema or chronic bronchitis.
Other restrictive lung diseases, such as interstitial fibrosis or pneumoconiosis, may also cause orthopnea. Additional causes of orthopnea may include acute respiratory distress syndrome (ARDS), abdominal obesity, ascites, pneumonia, or trauma to the nervous system.
How is orthopnea diagnosed?
To diagnose orthopnea, a healthcare professional may begin with a full medical history and physical exam. Questions such as how many pillows are used to sleep, the presence of chest pain or coughing, and exercise tolerance may reveal the underlying cause.
Additionally, the presence of wheezing, rales, or dullness to percussion on a pulmonary physical exam can indicate pulmonary involvement, while cardiovascular exam may reveal murmurs, abnormal location of maximal impulse, or additional heart sounds.
Because orthopnea is a symptom of another underlying disease, additional medical testing may be required to uncover the underlying cause. Blood tests, such as a complete blood count (CBC), arterial blood gas (ABG), and B-type natriuretic peptide (BNP), may be required to determine whether the individual has anemia, hypoxia (i.e., insufficient blood oxygen), or excess stretch in the ventricles, respectively.
Imaging, such as an X-ray, may also be utilized to visualize any fluid build-up in the lungs, while an echocardiogram can be used to visualize abnormalities of the cardiac anatomy. Spirometry may also be a useful tool if an underlying pulmonary disease is suspected. Additional testing may also be necessary to rule out other causes.
How is orthopnea treated?
Treatment of orthopnea should include treatment of the underlying cause. Treatment of the underlying cause is dependent on the disease and can vary. Pulmonary congestion may be treated acutely using diuretics (e.g., furosemide) to relieve the increased volume in pulmonary venous circulation. Heart failure can also be managed using diuretics, beta-blockers, and ACE inhibitors. Lung disease may be treated with bronchodilators, oxygen therapy, and glucocorticoids.
Orthopnea
Orthopnea is a symptom of congestive heart failure with failure of both ventricles and increased pressure from fluid through the pulmonary circulation. It is characterized by shortness of breath during low-impact activities or at rest. If in a prone or supine lying position, the patient must sit up or stand up for relief.
Two symptoms of orthopnea include:
-
Platypnea, shortness of breath while standing;
-
Trepopnea, shortness of breath while lying on the side.
Three variations of orthopnea include:
cardiac orthopnea, left- and right-sided congestive heart failure;
gestational orthopnea, heart failure, cardiomyopathy, and edema due to red blood cell lysis during pregnancy;
paediatric orthopnea, sudden infant death syndrome or asthma due to sleeping position.
Orthopnea causes include:
- heart disease;
- angina pectoris;
- ascites;
- upper respiratory tract infections;
- fear and anxiety;
- diaphragm paralysis;
- obesity;
- emphysema;
- pneumonia;
- COPD;
- pulmonary edema;
- pleural effusion.
The 5PLS for dyspnea
The scale includes the absence of dyspnea (a score of 1)
Conclusion from Dreducation.pk
1. How do you pronounce orthopnea?
Orthopnea is pronounced or-thaap-nee-uh.
2. What is orthopnea?
Orthopnea refers to difficulty in breathing that occurs when lying flat and is relieved by sitting or standing. This symptom often progresses over time and may require individuals to sleep with multiple pillows for relief. The need for more pillows, such as in “three-pillow orthopnea,” indicates more severe symptoms. Orthopnea is caused by pulmonary congestion, which affects the lung’s ability to expand, leading to shortness of breath.
3. What is the difference between orthopnea and dyspnea?
While both terms describe shortness of breath, orthopnea specifically refers to breathing difficulty while lying down, whereas dyspnea can occur in any position.
4. What causes orthopnea?
Orthopnea is most commonly associated with heart conditions, such as congestive heart failure, coronary artery disease, and valvular disorders. Other causes include chronic obstructive pulmonary disease (COPD), emphysema, and lung diseases such as pneumonia, interstitial fibrosis, and more.
5. How is orthopnea diagnosed?
Diagnosis of orthopnea involves a thorough medical history, physical exam, and tests like blood work, chest X-rays, and echocardiograms to determine the underlying cause.
6. How is orthopnea treated?
Treatment focuses on managing the underlying condition causing orthopnea. For heart-related issues, medications such as diuretics, beta-blockers, and ACE inhibitors are commonly used. For lung conditions, treatments may include bronchodilators, oxygen therapy, and corticosteroids.
Orthopnea is an important symptom that often signifies underlying cardiovascular or pulmonary issues. Accurate diagnosis and treatment are crucial for improving a patient’s quality of life.






